CMS Proposes Site-Neutral and 340B Reform
The Centers for Medicare & Medicaid Services (CMS) recently released its proposed Medicare Outpatient Prospective Payment System (OPPS) rule that includes welcome reforms to site-neutral payments and the 340B drug pricing program. The OPPS rule annually adjusts Medicare payment rates for hospital outpatient services paid for through Part B. We are thrilled to see a site-neutral payment policy included in the proposed rule that CMS estimates could save $7 billion over the next decade. It is also encouraging to see policymakers take on 340B drug pricing reforms, though it is unfortunate those savings are not allowed to go toward deficit reduction, which would be far preferable. Congress should build on CMS’s efforts by enacting a broader site-neutral policy, codifying and making permanent 340B reforms, and dedicating the savings to much-needed deficit reduction.
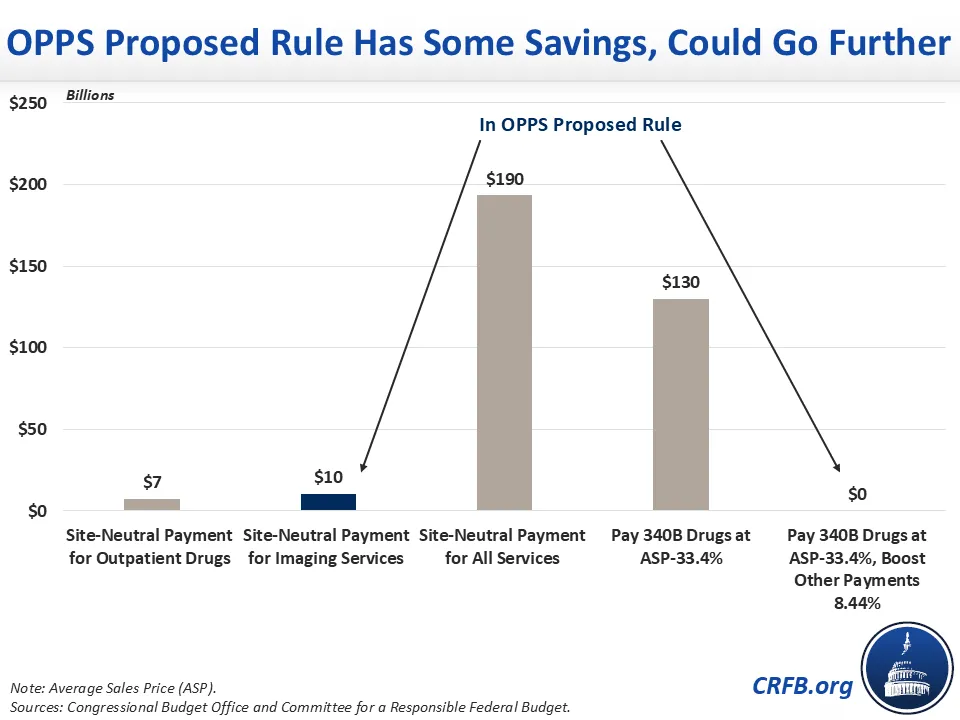
Under current law, Medicare pays more for Hospital Outpatient Departments (HOPD) than for the same service provided at an independent physician’s office; this practice raises Medicare costs for beneficiaries and the government and encourages excessive hospital consolidation. To address this, we and others have long supported moving to “site-neutral payments” for all services in Medicare, which could save the federal government almost $200 billion over a decade.
In the proposed OPPS rule, CMS would adopt these site-neutral payment rates narrowly for outpatient imaging services, such as X-rays. Experts agree this is an obvious place to implement site-neutral payment policy, as an X-ray should not cost more based on where you receive the imaging service. CMS estimates this policy could save Medicare about $7 billion over ten years. However, based on CBO's estimate, we estimate this would save Medicare about $10 billion over ten years while reducing beneficiary premiums and cost sharing by an additional $7 billion. This proposed rule builds on changes from last year, when the calendar year 2026 OPPS final rule implemented site-neutral payments for outpatient drug administration, saving the federal government about $7 billion over ten years and beneficiaries an additional $5 billion. Together, these two policies will reduce national health expenditures by almost $20 billion over a decade.
The 340B Drug Pricing Program was created in 1992 to help hospitals serving low-income communities by requiring drug manufacturers to sell to those hospitals at discounted prices. However, design flaws and poor incentives in the program have caused it to drive up health care costs and pay large windfalls to wealthy hospital systems as opposed to safety net hospitals. Hospitals are able to charge Medicare 6% above the Average Sales Price (ASP) of the drug even as hospitals purchase the drugs for a sharply discounted rate.
The proposed OPPS rule would address this price spread by reducing Medicare payment for 340B-acquired drugs to 33.4% below the ASP for calendar year 2027, based on the estimated price paid by hospitals on average. Using CBO estimates of a similar policy, we estimate this policy could save about $130 billion over a decade, if the policy was made permanent. However, due to budget neutrality requirements, in 2027 CMS would spend those savings on an 8.44% increase in payments to Part B non-drug services, leading to little or no net deficit reduction.
While CMS is right to improve incentives and reduce costs for the 340B program, doing so through the OPPS rule means that savings are recycled back to Medicare Part B payments rather than to help shore up Medicare amidst rapid cost growth. Instead of relying on CMS to address the problems with 340B drug pricing program, Congress should act to do so. This could include codifying and making the new 340B rule permanent without the higher hospital payments, a phase down of the higher hospital payments, or identifying alternative cost-saving reforms.
With high and rising health care costs, policymakers should ensure that any reforms to Medicare work to reduce overall spending in the program. It is welcome to see long-discussed reforms coming to fruition in Medicare, and we encourage CMS to keep site-neutral payments in the final rule and for Congress to go further to reform 340B and adopt broader site-neutral policies to reduce overall health care spending.
Note: Updated to clarify that the CMS 340B payment policy proposal is only for calendar year 2027.

