Equalizing Medicare Payments Regardless of Site-of-Care
Currently, the Medicare program pays higher rates for medical services performed in hospital outpatient departments (HOPDs) than it pays for the same services when they are performed at physicians’ offices or Ambulatory Surgical Centers (ASCs), even when the care is equally safe and effective. In order to lower health care costs for patients and the Medicare program, policymakers could consider changing this policy.
As part of the Health Savers Initiative, this paper presents a description and savings estimate for an option to equalize payments for a specific set of services across care settings in Medicare. This policy, often called site-neutral payment reform, has bipartisan support and has been recommended by the Medicare Payment Advisory Commission (MedPAC) and proposed by Presidents Trump and Obama.
This policy would not only save Medicare dollars and reduce Medicare premiums and cost-sharing, but it could also generate savings in other parts of the health system. Commercial payers could achieve savings by also adopting site-neutral payments given strengthened negotiating leverage from Medicare’s change. Furthermore, by reducing payment rates for HOPDs, there would be less incentive for hospitals to purchase physician practices to convert to HOPDs, which has led to higher private sector prices.
Over the next decade (2021-2030), this site-neutral payment policy could:
- Reduce Medicare spending by $153 billion
- Reduce premiums and cost-sharing for Medicare beneficiaries by $94 billion
Assuming different levels of private sector spillover savings, this policy could also:
- Reduce total national health expenditures by a range of $346 to $672 billion
- Reduce the federal budget deficit by a range of $217 to $279 billion
- Reduce private cost-sharing and premiums1 by a range of $140 to $466 billion
Given the high and rising costs of health care, a number of bold policy changes will be needed to assure long-term affordability and sustainability. In this context, paying the same rate for the same service regardless of site-of-care could be considered an obvious option, particularly because this policy has already achieved bipartisan support.
The Health Savers Initiative is a project of the Committee for a Responsible Federal Budget, Arnold Ventures, and West Health, which works to identify bold and concrete policy options to make health care more affordable for the federal government, businesses, and households. This brief presents an option meant to be just one of many, but it incorporates specifications and savings estimates so policymakers can weigh costs and benefits, and gain a better understanding of whatever health savings policies they choose to pursue.
The Case for Equalizing Payments
The Medicare program pays different rates for equivalent or identical services depending on where the service is performed. Generally, procedures performed in hospital outpatient departments are paid at a higher rate than the same procedures performed in a physician’s office or an ambulatory surgical center.
In some cases, the payment differentials are quite large. For example, Medicare pays HOPDs an average of 125 percent more than physicians’ offices for an evaluation and management (E&M or “clinic”) visit.2 And overall, Medicare rates for HOPDs are almost twice as high as rates for ASCs.3 These differentials exist in the private sector as well, as commercial insurers generally pay more for the same services when they are delivered in a HOPD than a physician’s office.
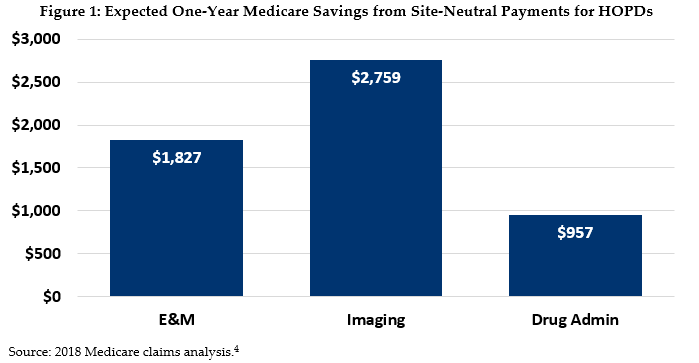
Using claims data, we find that paying HOPDs the same as other sites of care for equivalent, safely delivered services would generate significant budgetary savings for a variety of services (see Figure 1).
Historically, the rationale for higher payments to HOPDs relative to freestanding office settings was based on differences in regulatory burden, patient mix, and the complexity of services provided. Although outpatient departments used to be primarily located within a hospital (“on-campus”), many are now located off-campus, fueled in part by the purchase of independent physician practices by hospitals.
Higher payments are difficult to justify when offered to off-campus facilities that operate exactly the same as an independent physician’s office but are treated as HOPDs simply because they are hospital-owned. Often, hospitals purchase previously independent physicians’ offices largely to take advantage of the higher rate available by changing the office’s designation. In these cases, the exact same services are delivered by the exact same personnel, but at a higher cost to public and private payers.
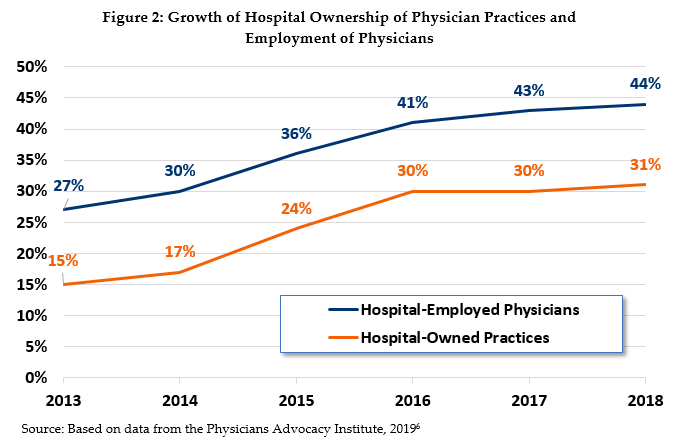
This situation has worsened in recent years. Between 2013 and 2018, the share of physician practices that were hospital-owned more than doubled. One-third of physician practices are now hospital-owned and hospitals employ 44 percent of all physicians (see Figure 2).5
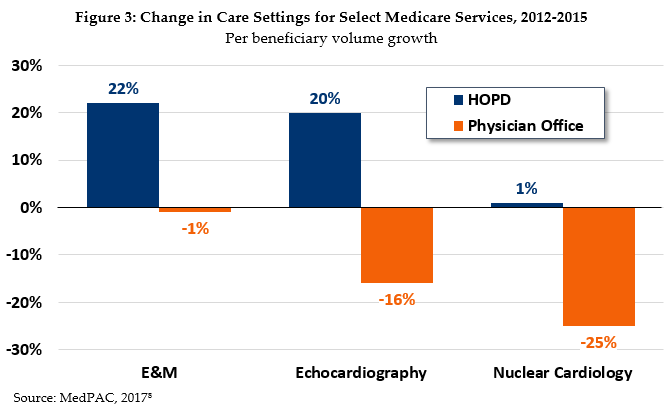
The increase in hospital purchases of physician practices has technically resulted in a shift in care settings from physician offices to HOPDs, but in reality, it has only increased prices for the same services (see Figure 3). Just looking at E&M visits, MedPAC estimates annual Medicare spending in 2017 was nearly $2 billion higher and beneficiary cost-sharing $480 million higher as a result of higher payments to HOPDs.
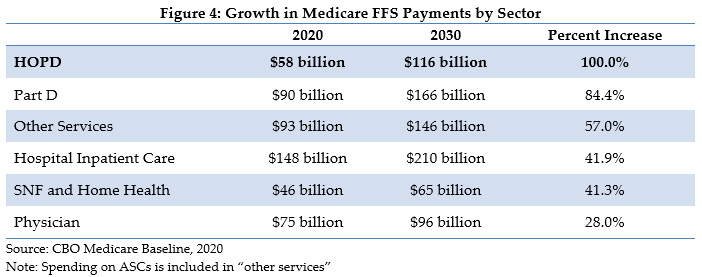
Overall, CBO has projected fee-for-service payments to HOPDs will grow faster than any other sector’s payments – doubling over the next decade (see Figure 4). By comparison, hospital inpatient care is projected to grow by 42 percent and non-HOPD physician services are projected to grow just 28 percent.
There is little reason for the significant payment differentials between HOPDs and physicians’ offices when the services performed are equivalent, are safely provided in office settings, and the patient health status is similar. This policy option would address the disparity and lower Medicare spending, lower premiums and out-of-pocket costs for beneficiaries, and reduce the financial incentives for vertical consolidation.
Recent Efforts to Make Payments Site-Neutral
In 2014, MedPAC issued recommendations to Congress and the Centers for Medicare and Medicaid Services (CMS) to enact site-neutral payments for a subset of hospital outpatient services. In particular, their criteria focused on services performed in physicians’ offices at least 50 percent of the time, not usually associated with an emergency department visit, and with relatively even patient severity between settings.
In 2015, Congress acted in part on these recommendations by passing the Bipartisan Budget Act of 2015. This bill established site-neutral payments for services received at off-campus HOPDs, but applied the policy only to future HOPDs. All current off-campus HOPDs, as well as those under construction, were grandfathered into the higher site-specific payments. Additionally, the law did not include site-neutral payment reforms for ASCs, stand-alone emergency departments, or on-campus HOPDs.
Since 2015, site-neutral payment policies have been part of every Presidential budget proposal under both President Obama and President Trump. In his most recent budget, President Trump proposed to apply site-neutral payments to all services provided at all off-campus hospital outpatient departments, eliminating the grandfathering provision of the 2015 law. In addition, the budget calls for site-neutral payments between on-campus hospital outpatient departments and physicians’ offices for services commonly performed outside hospital settings, such as E&M/clinic visits and imaging services. The President’s budget estimates $164 billion in savings for FY2021 through 2030.9
CMS attempted to administratively adopt site-neutral payments for all off-campus E&M/clinic visits, but implementation has been delayed by a series of lawsuits. Following a ruling in CMS’ favor, in December 2020 CMS implemented site-neutral payments for E&M/clinic visits at off-campus HOPDs in its annual outpatient prospective payment system rule for 2021. This analysis accounts for those savings in its baseline and examines additional opportunities to capture savings through site-neutral payments.
The Policy Details
This policy option would target HOPD services that are commonly and safely performed in physicians’ offices or ASCs and for which the patient mix is relatively equal, using criteria developed and recommended by MedPAC.
Medicare would pay for these services at the lower-cost, site-neutral rate. In addition to the services listed below, this option gives CMS authority to identify additional services eligible for site-neutral payments as delivery patterns emerge and technology advances. At minimum, the following services would be included:
- Certain services, including clinic visits, imaging, and drug administration performed at on-campus HOPDs would be paid at rates equivalent to those paid under the Medicare physician fee schedule (MPFS) that applies to physicians’ offices.
- Medicare payments for all off-campus (defined as 250 yards from the main hospital campus) HOPD services would be set at the MPFS-equivalent rate. Such payments would also apply to other types of off-campus facilities, including clinics and stand-alone emergency departments.
- Select procedures that are performed in Ambulatory Surgery Centers. Site-neutral payments would be extended to services that can be safely and appropriately performed in both HOPDs and ASCs.
If policymakers determine that higher payments for certain services are desired (e.g., for primary care), they could consider modest increases for specified services, but should still establish and maintain parity between different sites of service.10
Estimated Fiscal and Financial Impact
In order to estimate the impact of moving to site-neutral payments, we modeled the spending reduction that would result from applying the above payment changes. The Appendix outlines the methodology and assumptions used to generate these estimates.
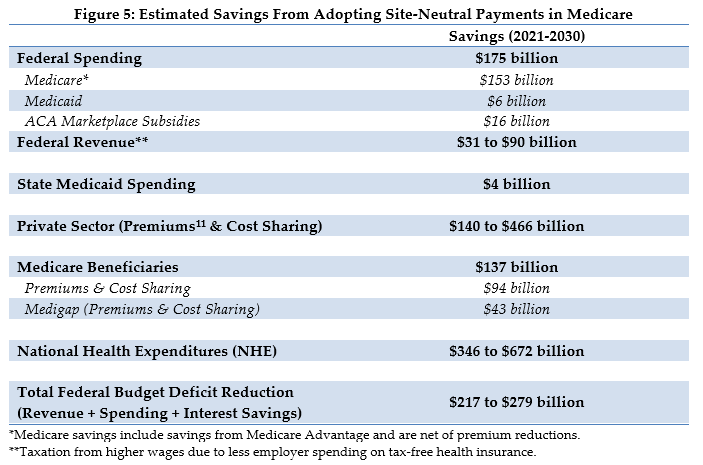
We estimate this policy change could result in $153 billion of net savings to the Medicare program over a decade. Medicare beneficiaries would save an additional $137 billion, including $51 billion in lower premiums and $43 billion in lower cost-sharing, plus an additional savings of $43 billion for those with Medigap coverage. Medicare’s overall spending on affected services would fall by roughly half once the policy is fully implemented.
These estimates assume the policy is implemented in Medicare and reduces spending in the private sector insurance market through two mechanisms: 1) encouraging broader adoption of site-neutral payment among commercial payers, and 2) reducing hospital incentives to acquire physician practices which has led to higher payment rates.
Overall, we estimate this option will reduce projected national health expenditures by a range of $346 to $672 billion over a decade and projected federal budget deficits by $217 to $279 billion.
Because there is insufficient information about how closely payment systems for private insurers mirror Medicare’s payment system, there is considerable uncertainty when estimating these spillover effects. However, we estimate those effects could be substantial under this option, with a potential range of savings between $140 to $466 billion in health costs outside of Medicare. Such savings would lower private health care premiums and increase taxable cash wages.12 For the federal government this could lead to between $31 to $90 billion in further revenue collection over the next decade.
Appendix: Estimating Methodology
The estimates in this document were produced through the joint effort of the partner organizations: The Committee for a Responsible Federal Budget, Arnold Ventures, and West Health.
The starting points for savings estimates were the March 2020 Congressional Budget Office baseline and the March 2020 National Health Expenditure projections from the actuaries at the Centers for Medicare and Medicaid Services. The Heath Savers Initiative will use this pre-Covid-19 baseline for all options to allow for the best comparisons because the full impact of Covid-19 on the baselines is unknown at this time.
The impact on the federal budget deficit was calculated by adding spending and revenue changes to interest cost savings estimated using CBO’s October 2020 interactive debt matrix.
This analysis uses two Medicare payment systems: the Medicare Physician Fee Schedule (MPFS) and the Outpatient Prospective Payment System (OPPS). The MPFS has two payment rates, one for services performed in outpatient settings (the facility rate) and one for services performed in physician offices (the non-facility rate). The non-facility rate under MPFS is higher than the facility rate because the fee compensates physicians for the additional expense of practicing in a freestanding office. When a beneficiary receives care in a hospital outpatient department, Medicare makes two payments, one through OPPS to the outpatient department for supplying the space, equipment, and staff and another through the MPFS to the provider who cared for that beneficiary. In most cases, the combination of the OPPS and MPFS payment for a service performed in a hospital outpatient setting is higher than the non-facility MPFS rate for services performed in a physician office. This analysis investigates how much could be saved by reducing higher OPPS payments so that the combination of the OPPS and the physician payments is equivalent to the MPFS non-facility payment.
The methodology was modeled on that used by MedPAC in its 2014 report to Congress. In order to develop modified OPPS rates for services frequently performed in facility settings,13 this methodology calculates differences between non-facility and facility payment rates from the MPFS. By replacing the facilities’ OPPS payments with these differentials, the facility MPFS payment, together with the new resulting OPPS payment, equals the non-facility MPFS payment, achieving site neutrality. The data used for this analysis was drawn from the 5% percent sample 2018 Limited Data Set (LDS) Medicare analytic files.
Services included in the proposal are divided into four groups:
- Evaluation and Management (E&M) Clinic Services – HCPCS codes 99201-99215 and G0463
- Preliminary Selected Ambulatory Payment Classifications (APCs)
- Additional APCs consistently performed in ASCs
- All other services performed in off-campus HOPDs.
Private sector spillover effects were estimated under three possible assumptions – 30 percent adoption of site-neutral payments by commercial insurers and employers; 50 percent adoption; and full adoption. There is evidence that commercial insurers follow Medicare’s lead on price changes, including one large study that found a $1.00 increase in Medicare price was correlated with a $1.16 increase in commercial prices for the same service.14 The extent to which decreases in prices from the private sector adoption of a Medicare site-neutral policy are less clear. Therefore, we present our spillover estimates as a range, rather than a point estimate.
1 As used in this brief, premium savings are calculated as savings on direct medical benefits and do not include administrative costs (“unloaded premiums.”)
2 MedPAC, “Report to Congress: Medicare Payment Policy," March 2019, Chapter 4. In 2018 HOPDs were paid $166 for the most common E&M visit for established patients compared with $74 for the same visit provided in a physician’s office. MedPAC and CMS use E&M or “clinic visit” at different times to describe similar interactions so in this brief we use both terms. https://www.medpac.gov/docs/default-source/reports/mar19_medpac_entirereport_sec.pdf.
3 MedPAC, “Report to Congress: Medicare Payment Policy,” March 2019, Chapter 5. In 2019, Medicare payment rates to HOPDs were 94% higher than those to ASCs for the same service. https://www.medpac.gov/docs/default-source/reports/mar19_medpac_ch5_sec.pdf?sfvrsn=0.
4 Analysis using the 2018 Medicare 5% sample; Imaging includes Levels 1-3 with contrast, Levels 1-4 without contrast, CT/CTA, MRI/MRA, ultrasound, and Levels 1-4 nuclear medicine; Drug administration includes Levels 1-4.
5 Physicians Advocacy Institute, “Updated Physician Practice Acquisition Study: National and Regional Changes in Physician Employment 2012-2018, “ February 2019, https://www.heartland.org/_template-assets/documents/publications/021919-Avalere-PAI-Physician-Employment-Trends-Study-2018-Update.pdf.
6 Physicians Advocacy Institute, “Updated Physician Practice Acquisition Study: National and Regional Changes in Physician Employment 2012-2018, “ February 2019, https://www.heartland.org/_template-assets/documents/publications/021919-Avalere-PAI-Physician-Employment-Trends-Study-2018-Update.pdf.
7 MedPAC, “Report to Congress: Medicare Payment Policy,” March 2019, Chapter 3. https://www.medpac.gov/docs/default-source/reports/mar19_medpac_ch3_sec.pdf?sfvrsn=0
8 MedPAC, “Report to the Congress: Medicare Payment Policy,” March 2017. https://medpac.gov/docs/default-source/reports/mar17_entirereport.pdf.
9 The CBO’s “Analysis of the President’s 2021 Budget” estimates the proposal saves $141 billion. March 2020. https://www.cbo.gov/publication/56278.
10 MedPAC. “Report to Congress: Medicare Payment Policy,” March 2018, Chapter 3. For example, there is evidence that E&M payments to physicians are under-reimbursed relative to other services and procedures. In 2018, MedPAC issued a recommendation for rebalancing the fee schedule toward Ambulatory E&M. https://www.medpac.gov/docs/default-source/reports/mar18_medpac_entirereport_sec.pdf.
11 Premiums excluding administrative costs, or “unloaded premiums.”
12 Economic theory says that when one part of employee benefits is reduced (health insurance costs) other benefits (wages) will increase. This shift in benefits results in additional federal revenue because premiums paid for health insurance costs are excluded from federal income and payroll taxes, but wages are not.
13 The analysis excludes the following entities: Ambulatory Surgical Centers (ASC), Critical Access Hospitals (CAH), Cancer Hospitals, Children’s Hospitals, ESRD Facilities, and Federally Qualified Health Center and Rural Health Centers (FQHC/RHC).
14 Clemens J and Gottlieb JD, “In the Shadow of a Giant: Medicare’s Influence on Private Physician Payments,” Journal of Political Economics, 2017 Feb; 125(1): 1–39, https://doi.org/10.1086/689772.


