Medicare Advantage in the Hot Seat
Recent actions from the Centers for Medicare & Medicaid Services (CMS) could help reduce the estimated $1.3 trillion in Medicare Advantage (MA) overpayments projected over the next decade. Specifically, CMS’s proposed rate notice would essentially flatline payment rates, while also reducing upcoding by eliminating “chart reviews” and making other technical changes. These changes could save the government $22 billion in 2027 alone, and should be allowed to go into effect as written in the proposed rate notice.
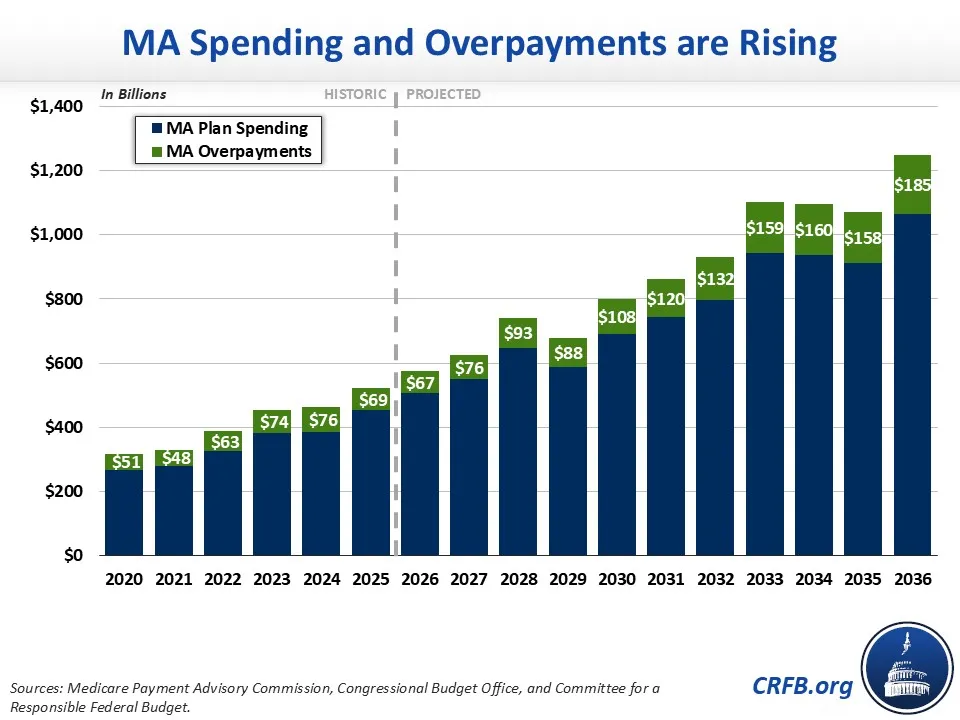
MA is a privately managed alternative to traditional Medicare. Although these plans have the potential to be more cost-effective than traditional Medicare, they end up costing the federal government far more – mainly because they take advantage of risk adjustments in their capitated payments, including by “upcoding” enrollees to make them appear sicker than they truly are. In total, the Medicare Payment Advisory Commission (MedPAC) estimates MA plans will be overpaid by about 14%, or $76 billion, in 2026.
To help address these overpayments CMS recently proposed only a 0.09% rate increase – which is far lower than last year’s 5.06% increase, or the 3.88% average increase over the past decade. In addition, CMS proposed to exclude diagnoses collected from “unlinked chart reviews,” a practice in which plans review members’ medical records to identify additional diagnoses without an actual doctor visit. CMS also proposes technical updates to the CMS Hierarchical Condition Category (CMS-HCC) Risk Adjustment Model (V28), incorporating more recent data from 2023 and 2024, improving the model’s accuracy.
Taken together, CMS estimates these changes could reduce Medicare costs by roughly $22 billion in 2027. We would expect more savings over time. As a result, these changes are likely to reduce deficits, improve Medicare Hospital Insurance (HI) trust fund solvency and lower beneficiary premiums.
The proposed rate notice would achieve these savings with a “belt and suspenders” approach. The near-freeze to overall payments would help offset large, broad-based overpayments that benefit MA plans. Meanwhile, the chart review and the V28 update would take a more targeted approach to overpayments. The removal of unlinked chart reviews could save up to $7 billion in 2027. As we have previously shown, modifications to the V28 model will save up to $15 billion in 2027.
Unfortunately, some special interests and opponents of MA reform have called for CMS to abandon these proposals and offer a significantly higher payment update.
Plans are unsurprisingly disappointed that the rate increase is not in line with the average over the past decade and have said they will be forced to cut supplemental benefits or increase premiums. However, many plans are offering benefits that have little to do with health care – with some even paying for pet food and golf fees – and evidence suggests modest reductions are likely to have little impact on even these benefits.
Other opponents of MA reform have criticized overpayment estimates from MedPAC – the legislative branch agency that analyzes Medicare data – arguing that MA enrollees are sicker than MedPAC believes and even supporting legislation that would prevent MedPAC from making favorable selection estimates. This is a classic case of “blaming the ref” – MedPAC is an independent, nonpartisan agency well known for its high quality and highly credible analysis. As we and many others have shown, it is well documented that individuals in MA plans are healthier than their counterparts in traditional Medicare. MedPAC’s estimate of a 14% net overpayment is in line with other estimates.
Of course, no estimate is perfect and actual MA overpayments could be higher or lower than MedPAC’s estimates. However, CMS’s policies as mentioned above would only close about a quarter of the estimated overpayment – meaning that MA plans will continue to be overpaid even if MedPAC is substantially overestimating current overpayment.
Given the very large size of estimated overpayments, policymakers should go further than CMS’s rate notice – for example by enacting the No UPCODE Act and/or the Reform the Medicare Advantage Program Act, increasing coding intensity adjustments, modifying Employer Group Waiver Plans and their star ratings, or using competitive bidding to set MA reimbursement rates.
There is far more work to be done, but CMS’s actions represent an important start. The Administration should stand by these reforms, and Congress should build upon them. Appropriately paying MA plans is one of the most efficient ways to reduce deficits, strengthen the Medicare HI trust fund, and lower health care costs.

