States Exploit SDP Grandfathering, Driving Up Medicaid Costs
The One Big Beautiful Bill Act (OBBBA) included important reforms to limit states’ costly use of State Directed Payments (SDPs) in the Medicaid program. However, recent actions to take advantage of the law’s “grandfathering” rules could undermine some of these reforms and prove quite costly. Two states alone have increased their SDP rates by 50% since OBBBA passed, costing the federal government roughly $20 billion over ten years. Closing this loophole could save tens of billions of dollars.
SDPs are supplemental payments that states make to Medicaid providers to compensate them for Medicaid’s low reimbursement rates. Unfortunately, some states have used these SDPs to increase payment rates far in excess of what is needed – often up to commercial rates – leaving the federal government with much of the bill. States have also used these SDPs in combination with provider taxes to significantly inflate their effective match.
In response to growing concern about the cost of SDPs, the OBBBA reconciliation law limited new SDP rates to Medicare rates (or 110% of Medicare rates in states that didn’t expand Medicaid under the ACA), and banned states from increasing SDPs above that rate.
To avoid disruptions to states and providers, OBBBA allows states to continue paying existing SDPs (referred to as “grandfathered” SDPs) at current higher rates through the end of 2027, and then phases down those payments gradually – by 10% per year until they reach Medicare (or 110% of Medicare) rates.
The Centers for Medicare & Medicaid Services (CMS) effectively broadened this grandfathering in a way that will allow far more spending on SDPs. While the law allows grandfathering for plans that start within 180 days of enactment, CMS instead chose to interpret this as 180 “business days.” This is a meaningful distinction, as it grandfathers through March 27, 2026 instead of December 31, 2025 – allowing new and increased payments at the beginning of the year (as many are) to pay far above Medicare rates, so long as applications were submitted before the law was enacted on July 4, 2025.
This seemly small change to the grandfathering rule comes with costly repercussions. The law currently allows states to pay SDPs up to the average commercial rate. Given the large difference between commercial and Medicare rates and slow phase-down rate for SDPs, allowing large payments to be initiated this year will increase federal costs for years to come. For example, Florida’s average commercial rate is 3.5 times Medicare rates. If CMS approves SDPs at that rate, it could take up to 10 years to phase down, depending on how CMS interprets the phase-down methodology.
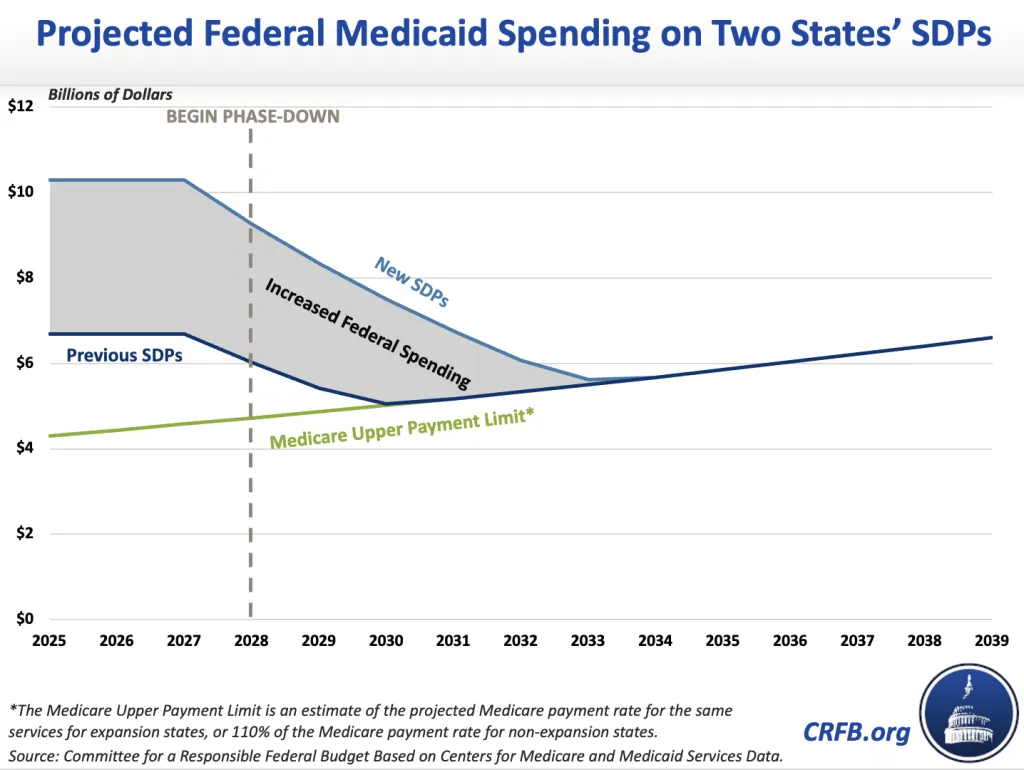
In just two states – Illinois and Texas – efforts to take advantage of CMS’ flexibility could drive up total Medicaid costs by nearly $40 billion over a decade and cost the federal government over $20 billon.
In its 2024 SDP cycle, Illinois was approved for $4.7 billion (federal and state) on SDPs for inpatient and outpatient providers. On September 9, 2025, after OBBBA was approved, CMS approved an SDP that the state submitted the previous May for an increase to $8 billion. Similarly, before OBBBA, Texas was approved to pay inpatient and outpatient providers SDPs totaling $6.5 billion. After OBBBA, CMS approved Texas’ SDPs to increase to $9.1 billion.
As a result of the increases, we estimate Texas and Illinois will pay providers $38 billion more over ten years than they would have if their SDPs had been held to the levels of the previous year. Of that amount, the federal government will pay approximately $22 billion.
While Illinois and Texas represent two states taking advantage of this grandfathering loophole, CMS is still working through a backlog of applications for SDP increases from a number of other states. For example, Florida has reportedly applied to double one of their SDPs from $3.4 billion to $7.9 billion, which would raise some hospitals’ payments to the average commercial rate. In Florida this amounts to 350% of Medicare rates.
In the near-term, these actions will increase federal costs above even pre-OBBBA levels, and remain in place until 2028. Over a decade, they could cost the federal government tens of billions of dollars or more.
In order to ensure OBBBA is successful in reducing these excessive payments in the Medicaid program, policymakers should work to close this loophole. This could be done by re-defining the grandfathered SDP periods as “calendar days,” putting limits on SDP approvals within the grandfathering window, or by accelerating the 10% annual phase out (for example to 30% annually). These changes could generate meaningful federal savings.
Policymakers should act before OBBBA’s Medicaid payment reforms are further weakened.


