Site-Neutral Payments Would Lower Private Health Costs, Encourage Competition
The Health Savers Initiative recently published “Moving to Site Neutrality in Commercial Insurance Payments,” which examines the market inefficiencies driven by payment differences based on site-of-care, regardless of safety or clinical effectiveness. We estimate that site-neutral policies in commercial insurance could reduce national health expenditures by up to $458 billion over the next decade while reducing the federal budget deficit by up to $117 billion.
Read the full brief here.
A project of the Committee for a Responsible Federal Budget, Arnold Ventures, and West Health, the Health Savers Initiative seeks to identify bold and concrete policy proposals to make health care more affordable for the federal government, businesses, and households. This new brief builds off the work of a prior brief, “Equalizing Medicare Payments Regardless of Site-of-Care,” which found that site-neutral payments in Medicare could save $150 billion over a decade.
In full, policies that encourage site-neutral payments in the commercial insurance market could:
- Reduce total national health expenditures (NHE) by up to $458 billion.
- Reduce commercial premiums by up to $386 billion and patient cost sharing by $73 billion.
- Reduce the federal budget deficit by up to $117 billion.
Hospital care is the largest single source of expenditures within the health care system, driven in large part by high prices. One factor behind those high prices is site-based payments that create incentives to provide services in higher-cost settings, generally hospital outpatient departments (HOPDs) instead of independent physician offices.
The brief examines price differences for common services that do not require additional resources and are safe to provide either in an HOPD or in a physician’s office.
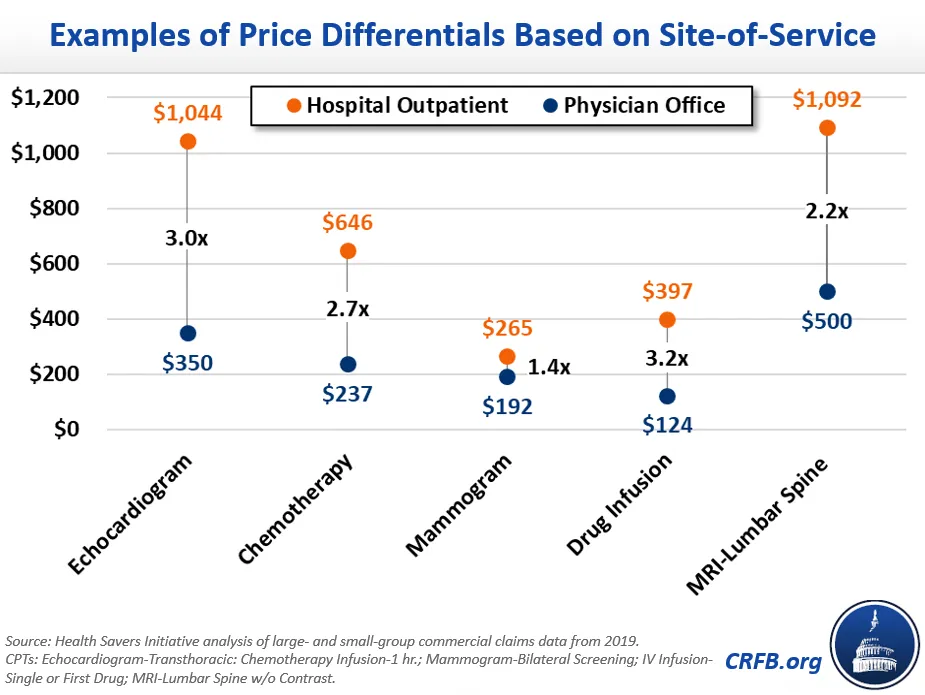
For these and many other services, the higher HOPD payments directly lead to higher out-of-pocket spending for patients and higher health care costs for the system writ large.
Importantly, these site-based incentives also encourage vertical integration – with hospitals purchasing physician practices and converting them to HOPDs to garner higher payments. This consolidation increases the pricing power of large hospital systems, enabling them to demand higher prices in negotiations with commercial insurers.
Moving the commercial market toward site-neutral payment policies would reduce NHE, allowing for lower premiums and cost sharing. With premiums falling, employers would also likely shift a share of worker compensation from non-taxable health care benefits to taxable wages, increasing government revenue.
This is the sixth brief published as part of the Health Savers Initiative. Other briefs have examined adopting site-neutral payments in Medicare, reducing overpayments in Medicare Advantage, capping hospital prices, injecting price competition into Medicare Part B drugs, and limiting evergreening for name-brand prescription drugs.
With health care spending growth being one of the top contributors to long-term fiscal uncertainty, this brief and the work of the Health Savers Initiative will inform policymakers of the options available to reduce cost growth while improving the efficiency and integrity of federal health care programs.


