Energy and Commerce Holds First Hearing on SGR
The House Energy and Commerce (E&C) Health Subcommittee yesterday held the first of two hearings on the Sustainable Growth Rate (SGR) formula for Medicare physician payments. Set to cut those payments by 21 percent in April 2015 when the latest "doc fix" runs out, the SGR will be one of the first "Fiscal Speed Bumps" the new Congress will confront this year. Fixing it permanently could cost at least $140 billion through 2025.
Yesterday's hearing focused on replacing the formula as well as whether and how to pay for the cost, featuring health care policy experts and policymakers. The session today featured representatives from various provider groups.
The witnesses at yesterday's hearing were:
- Former Senator Joe Lieberman (D/I-CT)
- Former OMB and CBO Director and current director of Brookings's Engelberg Center for Health Reform Alice Rivlin
- American Institutes of Research Institute Fellow Marilyn Moon
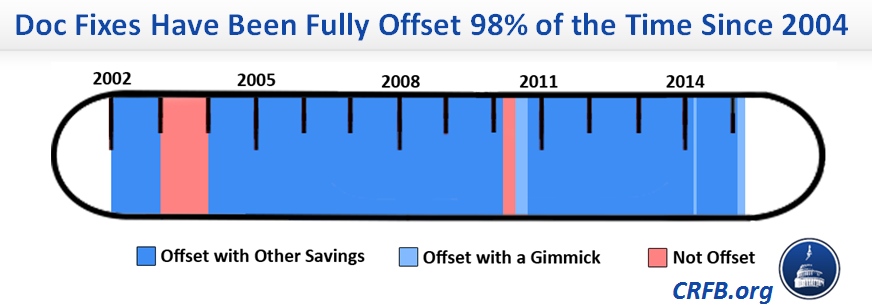
In their opening statements, both E&C Chairman Fred Upton (R-MI) and Health Subcommittee Chairman Joe Pitts (R-PA) encouragingly stated that repealing the SGR must be paid for, with Pitts citing CRFB's finding that doc fixes have been paid for 98 percent of the time since 2004.
Both noted that there exist numerous options with bipartisan support to pay for a replacement. Upton went further, calling on lawmakers to not just fix the SGR but make Medicare sustainable.
Senator Lieberman's testimony echoed Upton's in calling not just for a fully-offset SGR replacement, but also for a fully solvent and sustainable Medicare program -- and also trumpeted CRFB's analysis showing that doc fixes have nearly always been paid for, and have actually produced significant savings.

He pointed to a bipartisan proposal he made with Senator Tom Coburn in 2011, which the Medicare actuaries estimated would save $535 billion over ten years and move back the date of Part A's insolvency by 11 years. Their plan would reform cost-sharing and restrict Medigap plans from covering 1st-dollar costs (also part of our PREP Plan), increase and further means-test premiums, and raise the Medicare eligibility age to 67. He suggested that any part of this plan could be used or modified as offsets in an SGR fix or Medicare reform bill.
Dr. Alice Rivlin agreed with Lieberman that lawmakers would ultimately have to go further than just paying for the SGR to make Medicare spending sustainable, which she proposes to do primarily on using delivery system and provider payment reforms. She cited the February 2014 Brookings Institution plan, our PREP Plan, and the Bipartisan Policy Center's Health Care Cost Containment report as examples. She also suggested ways to improve the bipartisan, tricommittee bill to replace the SGR from last Congress by doing things like accelerating the use of alternate payment models and strengthening Accountable Care Organization programs. Finally, she stated that if Congress could not find enough offsets for a permanent SGR replacement, an acceptable fallback would be a "semi-permanent" fix of five years or so paired with structural reforms, and paid for with a policy like reducing subsidies for high-income Medicare beneficiaries (by further means-testing premiums).
CRFB's PREP Plan
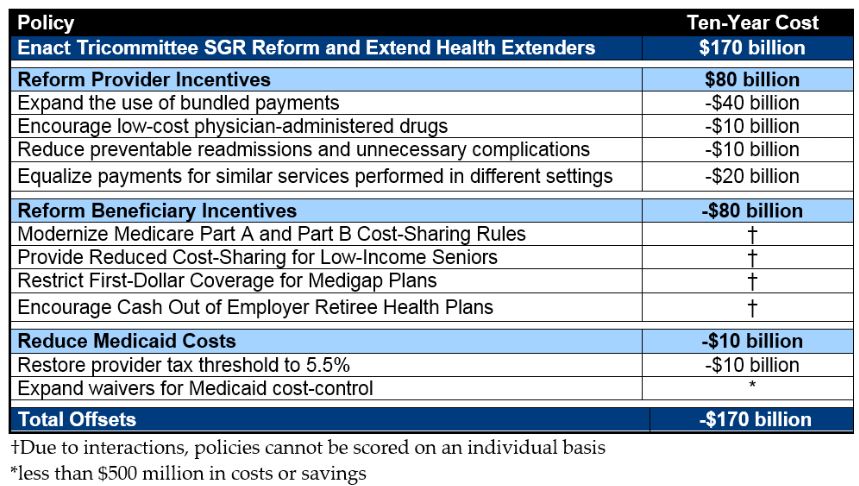
Dr. Marilyn Moon pushed back on suggestions that a doc fix should be paid for but said that if it is, the savings should not come from reducing benefits, either through premium, cost-sharing, or eligibility age increases. Although she made a brief nod to delivery system reforms, she suggested that offsets come from outside Medicare, such as a new revenue source, reducing tax loopholes, or cutting poorly-functioning programs. Notably, CRFB's PREP Plan to offset an SGR replacement would actually save money for Medicare beneficiaries.
Not surprisingly, each House Member at the hearing wanted to replace the SGR, but encouragingly, many of them expressed the need to pay for any fix. Lieberman underscored this point by saying that an unoffset bill would not pass Congress and that organizations pushing for that risk inaction. Others said that the SGR did not need to be offset because it was basically phony (despite the fact that it's achieved almost as much in savings as intended) or said that it could be paid for with the war spending gimmick.
In response to a question from Chairman Pitts, Lieberman explained that not offsetting a doc fix would ultimately be due to a lack of will, not options, making clear that there were countless plans out there including Simpson-Bowles and the President's budget that provide enough offsets. Rivlin added that the recent health care slowdown was no excuse not to offset a doc fix, and that making structural reforms could help ensure that the slowdown continues.
In response to a question from Subcommittee Ranking Member Gene Green (D-TX), Moon said that Congress would need to look at tax expenditures as a source of funding, as she said in her testimony.
Subcommittee Vice Chairman Brett Guthrie (R-KY) asked Rivlin for her opinions on specific offsets, and she responded that increasing means-tested premiums, reforming cost-sharing, and accelerating the move toward ACOs should be pursued.
Moon, responding to Rep. Kurt Schrader (D-OR), agreed that coordinating care, particularly when paired with improving recordkeeping, would be important to controlling costs. She also said that encouraging services to be delivered in the right setting is important, though it was not necessarily easy.
Rep. Gus Bilirakis expressed the need to put Medicare on sound financial footing for both future and current beneficiaries, asking Lieberman specifically about his proposal to modernize cost-sharing. Lieberman explained that the policy would both make cost-sharing much more understandable for beneficiaries and also help to limit overutilization (particularly with Medigap restrictions). Rivlin added that such proposals usually include a limit on out-of-pocket costs to protect beneficiaries.
In response to Rep. Larry Bucshon (R-IN) with regard to the consequences of doing nothing on the Part A Hospital Insurance (HI) trust fund, Rivlin said that lawmakers would likely act so those consequences would not be realized, but also made clear that the longer they waited, the more they difficult they would find it to solve because reforms could not be phased in as easily or taxes would have to be ramped up more quickly.
Full Committee Ranking Member Frank Pallone (D-NJ) asked whether the aging component of Medicare's expected growth meant that revenue would need to go up. Moon responded that it would and that gradual increases in payroll tax rates were anticipated at the beginning of the program.
Asked by Rep. Joseph Kennedy III (D-MA) about the prospects for the HI trust fund, Moon responded that she thought action would come soon because it had to: health care was very expensive, so there was urgency to get costs under control. She was optimistic about further action on pilot projects in the Affordable Care Act, with lawmakers taking what they've learned from these programs and applying them to Medicare to save money.
There was plenty of other discussion on paying for and replacing the SGR plus the prospects for slowing the growth of health care costs more broadly. The hearing is well worth a watch to see the assessment of where we stand on Medicare. Click here to see the hearing or watch the video below.


