The Physician Bonus and Medicare Sequester Suspension Should Not be Continued
A lobbying campaign recently began to extend two temporary COVID-era increases in Medicare provider payments – the Medicare sequester hiatus and temporary physician payment bonuses – beyond their December 31st expiration. Given the current state of the economy, lawmakers should ignore these calls and allow COVID relief to expire as intended. Extending these policies would cost roughly $18 billion for a one-year extension and $235 billion if made permanent, boosting Medicare premiums by an average of over $4 billion per year, and worsening existing inflationary pressures.
Canceling the restoration of the two percent Medicare sequester, which has been on a temporary hiatus for the last 20 months, could cost $15 billion over one year and $200 billion if made permanent over 10 years. Though the Medicare sequester originated as part of an enforcement mechanism to encourage the 2011 Joint Select Committee on Deficit Reduction (the “Super Committee”) to agree to a fiscal plan, it has proved an effective mechanism to reduce the cost of Medicare for beneficiaries and the federal government, and has been supported by lawmakers on both sides of the aisle. Lawmakers have extended the Medicare sequester seven times (most recently in the bipartisan infrastructure bill) so it is now in place through 2031 as opposed to the original 2021 expiration date.
(Importantly, the Medicare sequester differs from the PAYGO sequester, which would require an additional 4 percent cut to Medicare payments (and 100 percent cut to certain non-Medicare programs). Lawmakers should allow the 2 percent Medicare sequester to go into effect as scheduled and intended, but could replace the 4 percent PAYGO sequester with responsible alternatives.)
Extending the 3.75 percent Medicare physician bonus will cost another $3 billion to do for one year and $35 billion to continue over ten. The temporary bonus was enacted in the bipartisan Response & Relief Act passed in December of 2020. The purpose was to assist physicians struggling from the loss of business during the pandemic shutdowns and to ease the transition to a years-in-the-making policy change to rebalance physician payments towards primary care.
Cost of Extending Medicare Provider Payments
| Policy | 1 Year Cost | 10 Year Cost |
|---|---|---|
| Suspending Medicare Sequester | $15 billion | $200 billion |
| Extending Physician Bonus | $3 billion | $35 billion |
| Total Cost of Extensions | $18 billion | $235 billion |
| Memo: Beneficiary Premium Increases | $3 billion | $45 billion |
Sources: Congressional Budget Office and Committee for a Responsible Federal Budget. Estimates are rough and rounded.
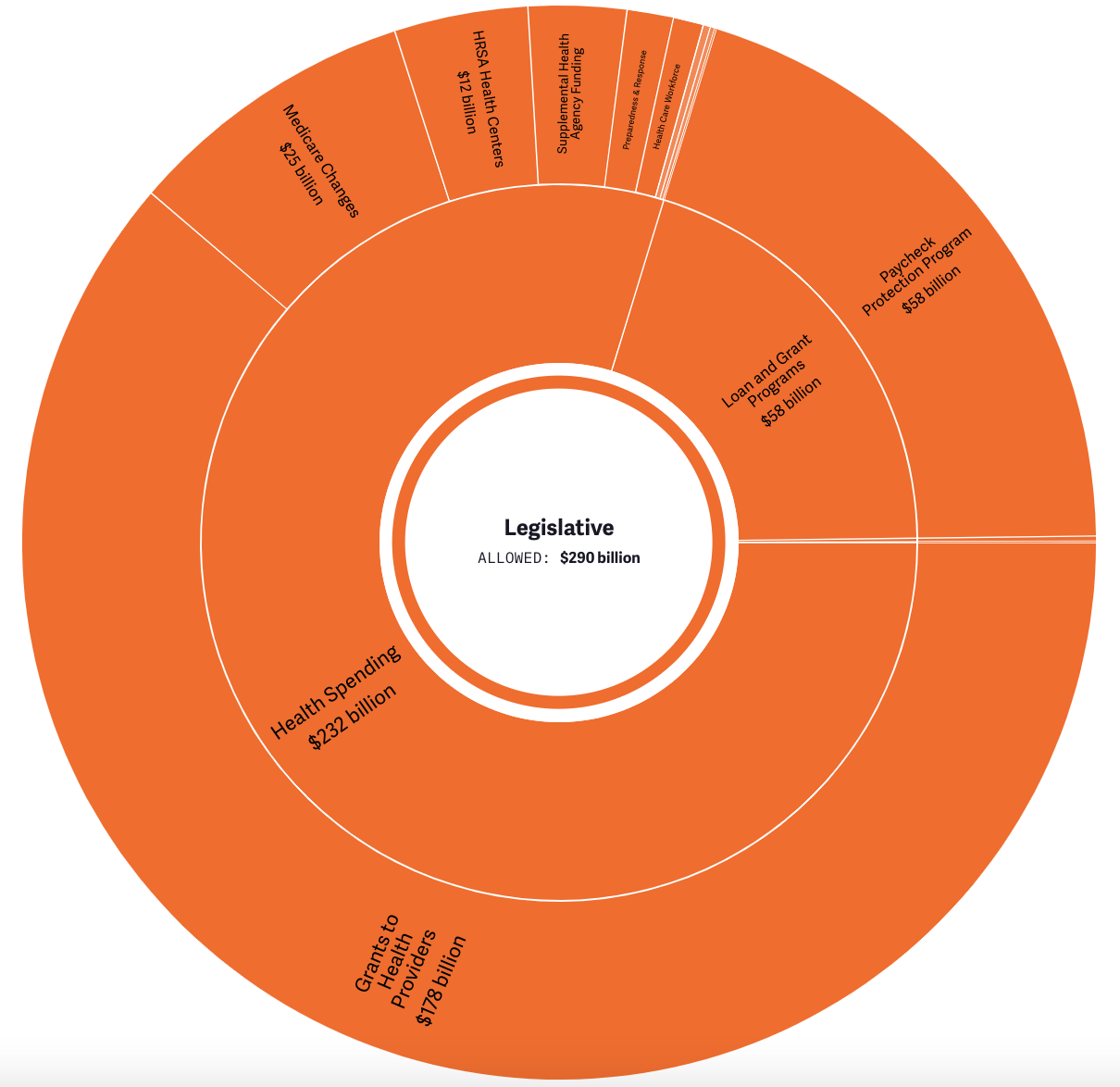
There is little reason to extend either the sequester hiatus or physician bonus in full. Lawmakers have already allocated nearly $300 billion directly to health care providers, in addition to spending roughly $150 billion to assist Americans in getting health care and providing health care providers with another $100 billion of “Advanced Payment” loans.
Elective procedures and in-person visits have largely normalized at this stage, while hospital revenue has returned to trend (and is higher than pre-COVID). From a macroeconomic perspective, the economy has largely (though not fully) recovered and is no longer in need of further stimulus. Instead, the economy currently faces high rates of inflation, which higher Medicare payments would exacerbate.
Though advocates have described the expiration of the physician bonus and sequester hiatus as a “substantial cut,” in reality it simply represents a return to normal and the end of one-time COVID relief payments. Households and businesses do not expect further Economic Impact Payments or Payroll Protection Program loans next year – and the end of this temporary relief is not considered a cut. There is no reason a different set of rules should apply to health care providers.
Overall, allowing sequester suspension and the physician bonus renewal could set the stage for an indefinite sequester suspension and further increases in Medicare provider payments. This would be a huge mistake for a program already facing an unsustainable future over the long term and Medicare Hospital Insurance trust fund insolvency in just five years.
If lawmakers view the change in Medicare provider payments as too abrupt or support higher overall payment levels, they should develop thoughtful reforms to transition to a new system and come up with offsetting spending reductions or revenue increases to pay for them. There is no justification for deficit financing Medicare spending increases, nor the extension of any other COVID relief.
From the debt limit to the PAYGO sequester, Congress has several major issues to address before the end of the year. They don’t need to create more work for themselves by extending policies that should be allowed to expire as intended.
Direct COVID Relief for Health Providers