Strategies to Lower Health Care Prices from KFF
Although most federal health spending goes to Medicare and Medicaid, the government is projected to lose over $350 billion of income and payroll tax revenue this year as a result of tax-excluded private health insurance premiums, and spending roughly $90 billion more on ACA insurance subsidies. A recent Kaiser Family Foundation (KFF) report discusses ways to lower the cost of these private plans by reducing health care prices in the private insurance market.
Lowering private-sector health care costs not only reduces premiums and out-of-pocket costs but deficits as well. The Committee for a Responsible Federal Budget's Health Savers Initiative has discussed numerous policy options that reduce private insurance premiums and deficits, with every $100 billion of premium reductions translating into upwards of $25 billion of income tax revenue.
In the KFF report “Price Regulation, Global Budgets, and Spending Targets: A Road Map to Reduce Health Care Spending, and Improve Affordability," Maximilian Pany, Jeannie Fuglesten Biniek, and Tricia Neuman highlight a number of options to address the high prices paid by private insurance. They suggest that now is an especially important time to look for government intervention in pricing because of “decades of sustained consolidation and rising prices in the health care sector call into question the ability of commercial insurers and employers to control increases in health care prices on their own.”
In recent years especially, prices paid by private insurance plans have grown substantially faster than those paid by Medicare. According to the Congressional Budget Office, from 2013 to 2018, spending per person from private insurance plans grew by 3.2 percent per year, compared to 1.8 percent in Medicare. The entire difference can be explained by prices, which rose 2.7 percent annually in private plans compared to 1.3 percent annually in Medicare.
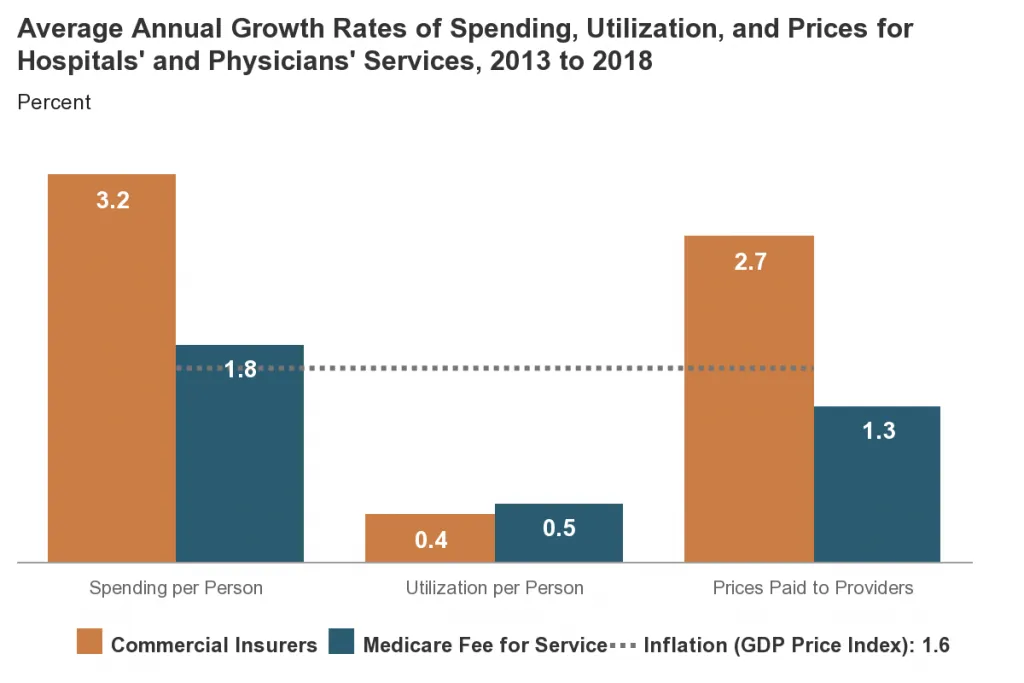
Source: Congressional Budget Office.
The KFF study surveyed several proposals to lower private sector price levels, including direct price regulation, global budgets, and spending growth targets as ways to reduce the growth of health care spending.
The three options for direct price regulation explored by KFF, include directly setting prices, creating price caps, or creating price growth caps. Price setting implements a fixed price for a particular service, such as Medicare’s fee schedule, and is mutually exclusive from the price caps and price growth caps. Price caps limit the maximum price that a provider can charge but allow market forces to work below the cap. They can target all prices or just out-of-network prices (for more on how these options work, see this analysis published earlier this year in Health Affairs).
Our Health Savers Initiative analysis, Capping Hospital Prices, explored one version of this price cap that would limit commercial hospital prices to 200 percent of Medicare prices. Even while continuing to allow private insurance to pay up to twice what Medicare does, we found the proposal would reduce national health expenditures by $1 trillion over a decade and reduce budget deficits by over $200 billion.
The KFF analysis also explores global budgets, which involves limiting spending to a set amount for a specified population. Global budgets can be structured as either a voluntary arrangement where providers receive fixed amounts for certain populations or on a mandatory basis, where all payers must participate. KFF cites the Maryland hospital system’s global payment model as a mandatory arrangement example that has demonstrated an ability to reduce expenditures for some beneficiaries. The predictable revenue stream from a global payment model makes it resilient and well suited for emergencies, such as COVID-19. KFF concludes that modest savings can be achieved using voluntary budget contracts while maintaining quality.
Lastly, KFF considers total spending growth targets, which place limits on increases in health expenditures over a period of time at the insurer, provider, or market level. The primary policy consideration is determining the growth benchmark index, similar to the consideration with price growth caps. Spending growth targets can also be structured to be mandatory or voluntary and can work in conjunction with other spending constraint mechanisms.
Many of these policy considerations could be implemented at either the national or state level. However, KFF points out that one of the major hurdles for state experimentation with new constraint policies is the Employee Retirement Income Security Act. This law prevents states from imposing new requirements on self-funded health plans, which include 64 percent of workers with employer-sponsored insurance. Self-funded plans may only be regulated at the federal level.
Although the KFF study does not estimate savings from these various proposals, they could be significant. As an extreme example, private insurance would cost about $350 billion (41 percent) less in 2021 if they paid Medicare prices, according to a separate KFF study. While most policy options under discussion to lower private health care costs would save far less than that, they could nonetheless make significant progress toward lowering premiums, out-of-pocket expenses, and federal deficits.
As health care costs continue to rise, both national and state policymakers should consider these types of proposals to slow the growth in health care spending and pass savings along to beneficiaries and taxpayers.


