American Health Care: Health Spending and the Federal Budget
The United States spends more on health care than any other country in the world, and a large share of that spending comes from the federal government.
In 2017, the United States spent about $3.5 trillion, or 18 percent of GDP, on health expenditures – more than twice the average among developed countries.
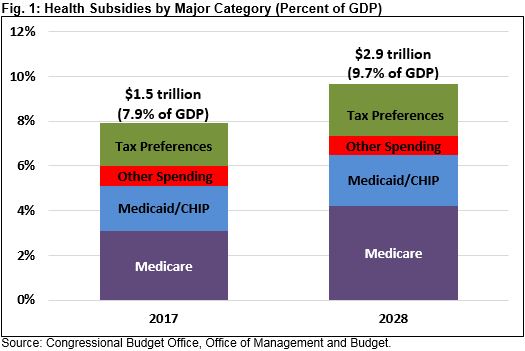
Of that $3.5 trillion, $1.5 trillion, is directly or indirectly financed by the federal government. In other words, the federal government dedicates resources of nearly 8 percent of the economy toward health care. By 2028, we estimate these costs will rise to $2.9 trillion, or 9.7 percent of the economy. Over time, these costs will continue to grow and consume an increasing share of federal resources.
Over the long term, the rising cost of federal health care spending is clearly unsustainable. Without a course correction, the result will be program insolvency, crowding out of important public priorities, and a growing federal debt.
Given how central health care spending is to the federal budget, it is important to understand how that spending is distributed and how it will grow. This paper will provide background on major health care programs in the federal budget. It is the first in a series called the American Health Care initiative, a joint collaboration of the Committee for a Responsible Federal Budget and the Concerned Actuaries Group.
The Rise of Federal Health Spending
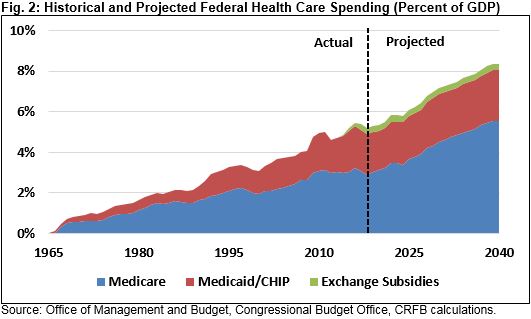
Federal health spending has grown significantly over the past several decades and is projected to grow in the future. Spending on the major federal health programs – Medicare, Medicaid, the Children’s Health Insurance Program (CHIP), and the health insurance exchange subsidies created under the Affordable Care Act – has increased from 0.8 percent of the economy in 1970 to 3.1 percent by 2000 and 5.4 percent in 2017 (total federal resources dedicated to health care, which include tax benefits as well, total about 8 percent of the economy). In dollar terms, major federal health spending has grown by 230 percent since 2000, while economy-wide prices have only risen 40 percent, and the economy has only grown by 90 percent. This growth is due to both automatic growth in enrollees and health care costs as well as health care expansions in the form of the Medicare prescription drug program and the Affordable Care Act.
As the population ages and per-capita health care costs rise, nearly all forecasters expect federal health care spending to continue to grow. Based on Congressional Budget Office (CBO) projections and our own extrapolations, major federal health spending will rise from 5.4 percent of GDP in 2017 to 6.8 percent in 2028 and 8.4 percent by 2040.
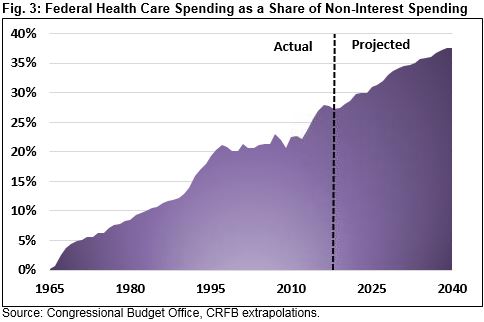
Meanwhile, health care will consume a larger share of the budget over time. In 1970, major health programs made up only 5 percent of the budget. That share increased to 20 percent by 2000 and 28 percent by 2017. By 2028, one-third of federal dollars not spent on interest will go toward health spending, and by 2040, nearly 40 percent will. Even these estimates do not account for the erosion of the tax base resulting from the tax exclusion for employer-sponsored health insurance.
In other words, the rising cost of health care is crowding out almost everything else.
Where Does the Money Go?
Most federal health care resources go toward financing four items: Medicare, Medicaid, the tax exclusion for employer-sponsored health insurance, and the exchange subsidies established under the Affordable Care Act. These and other programs are discussed below.
Medicare
Medicare is the largest federal health care program, serving 58 million elderly and disabled people at a gross cost of $702 billion in 2017 and a cost net of premiums of $591 billion. Medicare consists of three programs: Part A covers hospital and inpatient care, Part B covers physician and outpatient care, and Part D covers prescription drugs. Part A is funded primarily by a payroll tax while Parts B and D are funded through a combination of premiums and general revenue. Medicare beneficiaries may enroll in some or all of these parts or in private insurance known as “Medicare Advantage” while still receiving a similar federal subsidy.
Medicare costs are expected to rise rapidly in the coming years. In dollars, net costs are projected to more than double over the next decade to $1.3 trillion in 2028. This growth is due to both the aging of the population – the number of beneficiaries will rise from 58 million to 77 million – and growth in per-capita health spending – cost per beneficiary is projected to grow from $10,200 to $16,400. Both factors will continue to grow beyond the end of the decade.
Medicaid and CHIP
Medicaid is a state-run and jointly-financed health insurance program serving lower-income residents – including those making up to 138 percent of the poverty level in states that expanded Medicaid under the Affordable Care Act. Medicaid provides benefits for both acute and long-term care, covering nearly 100 million people over the course of a year. The Children’s Health Insurance Program (CHIP) is a similarly structured program that covers almost 10 million children in a given year.
The federal government pays for 50 to 75 percent of base Medicaid costs, depending on the state, and 90 percent of costs for the expansion population. On average, the federal government provides about 65 percent of total funding for Medicaid and 88 percent for CHIP, though CHIP’s share will fall to 65 percent by 2021. The two programs cost $391 billion in 2017 and are projected to cost $670 billion by 2028.
Exchange Subsidies and Other Spending
Other spending on health insurance or health care totaled $167 billion in 2017. This category includes subsidies for insurance purchased on the exchanges ($48 billion), veterans’ health care provided through the Department of Veterans Affairs ($70 billion), and health care for active-duty military and their dependents ($49 billion).
The exchange subsidies are projected to nearly double over the next decade due to large premium increases in the near term and general health care cost growth in later years. Both military health care and veterans’ health care are discretionary programs, meaning that they are appropriated each year rather than allowed to function automatically and currently are constrained by overall caps on discretionary spending. We estimate that these three areas will increase to a total of about $250 billion by 2028.
The Employer-Sponsored Health Insurance Exclusion and Other Tax Benefits
The tax code also provides several subsidies for health care and insurance. By far the largest is the exclusion for employer-provided insurance, which the Office of Management and Budget (OMB) estimates to have cost about $340 billion in 2017. An estimated 156 million people, a majority of the non-elderly population, receive coverage through their or their family’s employer. The exclusion is indirectly limited by the 40 percent “Cadillac” tax on high-cost insurance plans, but that tax will not go into effect until 2022 and has already had its start date delayed twice. Though the total number of people receiving employer-sponsored insurance is expected to fall slightly over the next decade, the cost of the subsidy will increase to nearly $650 billion by 2028 as health care costs rise (or higher if the Cadillac tax is repealed or further delayed).
Other tax subsidies totaled about $25 billion in 2017 and will grow to nearly $55 billion by 2028. The largest of these benefits is the medical expense deduction, available only to taxpayers who itemize their deductions and have medical expenses that exceed 7.5 percent of their income (or 10 percent after 2018). The cost of this deduction was $10 billion in 2017 and will increase to $20 billion by 2028. Other subsidies include the premium deduction for the self-employed ($8 billion in 2017, $12 billion in 2028), the deduction for contributions to Medical or Health Savings Accounts ($8 billion in 2017, $20 billion in 2028), and tax-free distributions from retirement plans to pay for premiums (less than $1 billion per year).
Rising Health Costs Threaten Trust Fund Solvency and Fiscal Sustainability
Rising health care costs represent a threat to both the Medicare program and the federal budget more broadly.
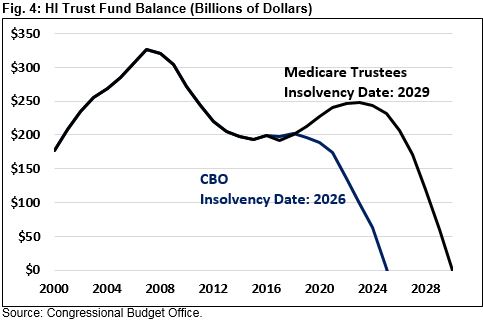
Medicare Part A is funded through the Hospital Insurance (HI) trust fund, which is financed primarily with a 2.9 percent payroll tax, split between employers and employees (an additional 0.9 percent high-income surtax and partial taxation of Social Security benefits provide additional funds). Currently, Medicare Part A costs and revenues are roughly equal, but costs are growing more quickly. As a result, CBO projects the Medicare Trust fund will be depleted by 2026, and the Medicare Trustees project insolvency by 2029.
Ensuring Medicare solvency will require closing a gap in excess of $100 billion per year by the end of the decade and equal to 0.64 percent of payroll over 75 years. That’s the equivalent of immediately increasing revenue by 16 percent or reducing spending by 14 percent.
Failure to address the costs of Medicare Part A will ultimately mean a 10 to 15 percent benefit cut, as benefits are limited to trust fund revenue. Other federal health programs have no similar constraint.1 Instead, rising health care costs will result in increased federal borrowing and are a key contributor to the unsustainable rise of the federal debt.
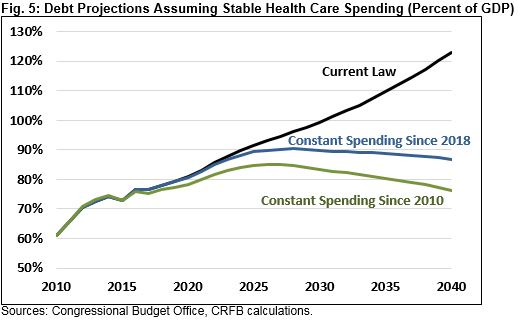
In fact, absent rising health care costs debt would roughly stabilize as share of the economy. Under current law, we estimate debt held by the public would rise from about 77 percent of GDP today to 96 percent by 2028 and 125 percent by 2040. If most major health care spending were held constant as a share of GDP after 2018 and HI trust fund spending were brought in line with revenue, debt would peak at about 90 percent of GDP in 2028 and fall slightly to 87 percent by 2040.
Had federal health care costs remained stable since 2010, debt would total 85 percent of GDP by 2028 and fall to about 75 percent by 2040.
Conclusion
Health care spending is already a large part of the federal budget and is projected to grow further over the long term. Medicare, Medicaid, CHIP, military health care, individual insurance, and health tax preferences for employment-based insurance already totaled 7.9 percent of GDP in 2017 and will grow to 9.7 percent by 2028. This growth has important implications for the budget, as health spending will become a larger share of budget and at least partially drive the growth in debt projected in the future. Controlling health spending should be a central part of the agenda to get federal debt under control.
This paper is part of the American Health Care Initiative, a joint collaboration of the Committee for a Responsible Federal Budget and the Concerned Actuaries Group dedicated to informing the public, policymakers, and key stakeholders regarding the fiscal and managerial challenges confronting our health care system. As part of the initiative, the two organizations will each publish and promote a series of papers, briefings, presentations, and other materials intended to energize a much needed conversation about improving the sustainability and accessibility of our health care system and managing the rising costs that threaten our current system.
1 Medicare Part B and D have trust funds, but they are replenished from the general fund annually and thus provide no real constraint.

